How can a palate be expanded?
There are three main options for expanding a palate:
ALF (Alternative Light-wire Functional): a very light wire appliance that exerts a subtle force over time, attracting the tongue to the roof of the mouth, and encouraging a stable swallow pattern. The ALF is adjusted both by the action of the tongue during the swallow, as well as by the dentist every 3-6 weeks.
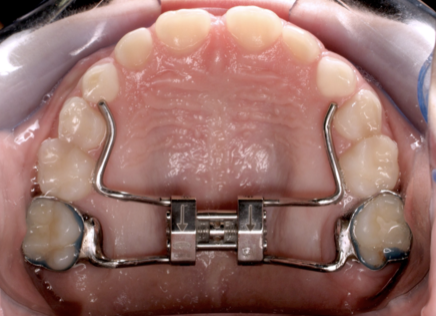
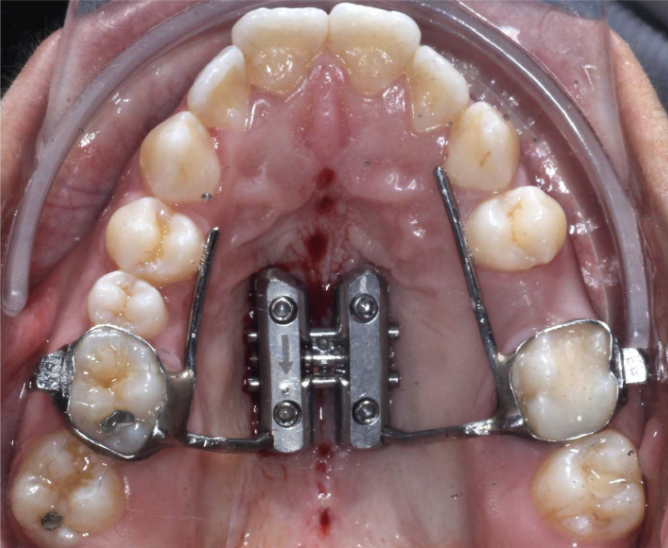
RPE (Rapid Palatal Expander): a rigid semi-customized appliance frequently bonded to a right and left molar, with hardware in the palate space, often blocking the tongue. These are expanded by the patient or parent weekly using screw-turns or occasionally directly by the dentist.
MSE (Maxillary Skeletal Expander): similar to RPE, the hardware is bonded to molars and activated in a similar way, but the MSE also requires implants to be screwed into the patient’s hard palate (and sometimes the hard palate itself is surgically punctured to speed up the process)
ALF (Alternative Light-wire Functional) applianceRPE (Rapid Palatal Expander)MSE (Maxillary Skeletal Expander)Why don’t you use rapid palatal expanders?
Dr. Caughey is naturally a very gentle person who loves working with children. Besides being gentle in general, the ALF process respects the patient’s need for sutural homeostasis. The midline palatal suture is not a straight line – and expansion does not happen in a linear way. The midline palatal suture connects from the left and right sides like tectonic plates; when the subtle pressure of the tongue presses on this suture, the midline opens at such a small increment that bone can easily fill the gap as it goes.
We have some concerns about RPE and MSE. If the expansion occurs without the function occurring simultaneously (because the hardware of these appliances block that very function), who’s to say the function will come online after treatment? Also, due to the non-linear nature of expansion, a rigid appliance can create asymmetry in the cranial vault – problems from this may not show up until lateral in life, in the form of migraine, dizziness, vision distortion, etc.
Further, sudden or drastic change can cause dissociation for the patient; what we seek is for the process to be integrating of the patient’s face, bite, and health. This doesn’t mean the RPE or MSE treatment is wrong, as there are certainly plenty of children who have experienced this type of care and withstood it well. But since we don’t know which children are resilient enough to handle heavy forces, we don’t risk it – we treat everyone gently.