Children rarely have TMJ problems until puberty is over. Most clicking and popping of the jaw joints (TMJ) does not show up until around age 15 in girls or 16 in boys. However, there are many “silent” TMJ joints needing management during the adolescent years, well before symptoms show up.
What’s Happening:
The mandible (lower jaw) experiences its biggest growth spurt in the same years as the long bones (arms and legs) – during adolescence. However, if the maxilla (upper jaw) is too narrow, the upper molars can restrict the forward development of the lower jaw and thus, the lower jaw does not achieve its full growth potential.
In addition to the narrow width of the maxilla, the lower jaw may not fully grow if there is a significant disruption of the ligaments attaching to the TMJ.
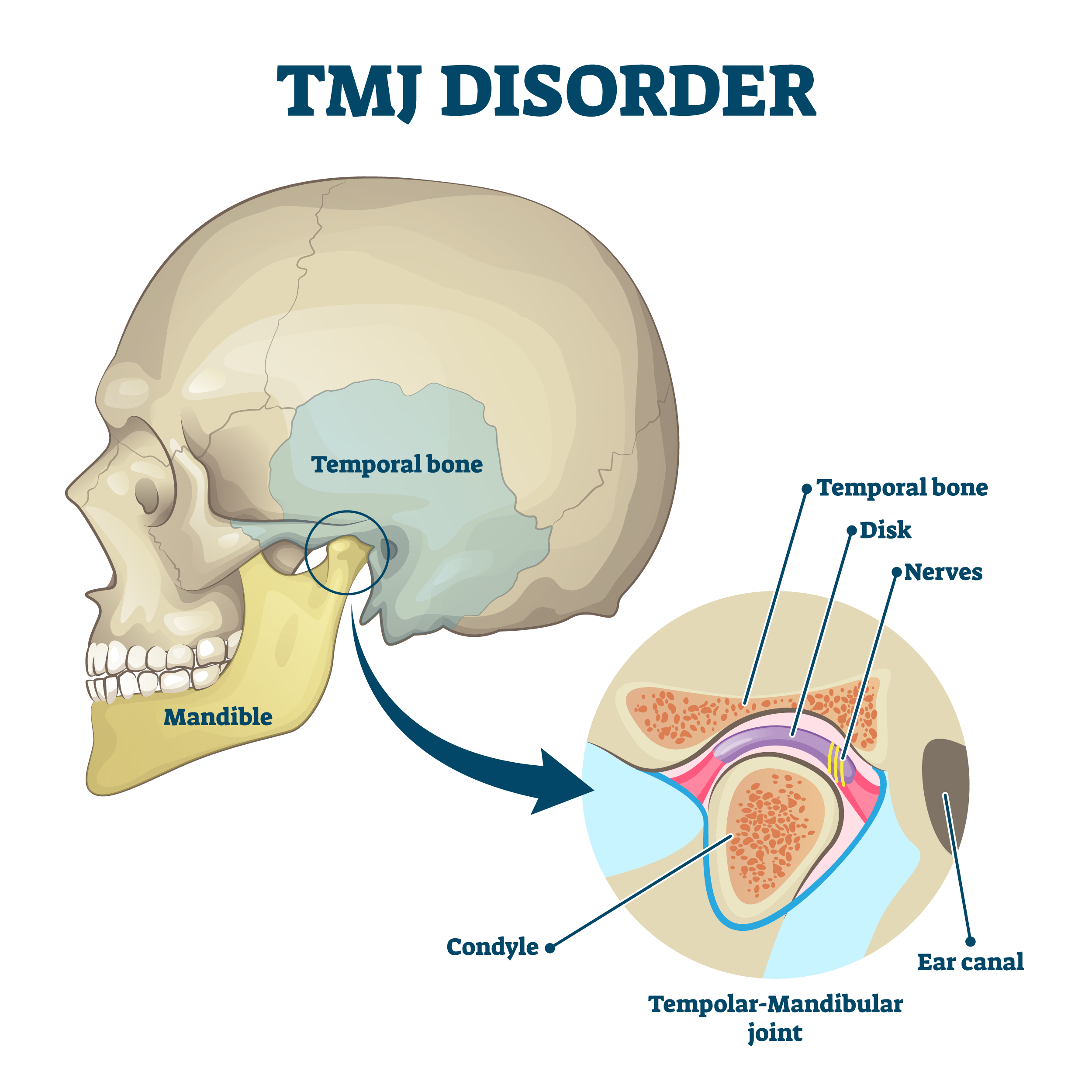
The TMJ is similar to a ball and socket type of joint, but is unique. The cushion for the TMJ is called a disc. That disc is a fairly tough anatomical feature that attaches to the bones comprising the TMJ (T for temporal, M for mandible). In a healthy joint, the disc glides along the slope of the temporal bone (socket) along with the mandibular condyle (ball).
In many cases, there will be one or more of the ligaments that attach the disc to the condyle that become stretched out or otherwise disrupted, and the result is a click or a pop that occurs during the opening and closing of the jaw. By itself, this click or pop is usually painless and does not cause problems during eating or speech or other normal function. If the child is growing fairly symmetrically in spite of this click or pop of the TMJ, it is likely that the disruption of the TMJ attachments is mild and does not need active management during adolescence.
A more severe disruption of the TMJ ligaments can result in an child’s face growing more asymmetrically during the pubertal growth spurt. While there are other factors that contribute to asymmetry of a face, the TMJ should always be closely studied prior to any treatment such as orthodontics, including palatal expanders. It is possible that orthodontic treatment using rigid appliances like rapid palatal expanders can exacerbate the asymmetry in spite of efforts to get the child’s face growing. If the disc is completely untethered from the condyle and has a complete displacement from the bony housing, treatment is needed as early as possible. That is because the growth plate of the mandible is the head of the condyle, and if the disc is not positioned correctly, the nutrients needed for growth are not getting to the growth plate.

What Needs to Happen:
In order to get the the mandibular growth back on track, it is necessary to position the mandible so that it slides back under the disc. This is often done with a removable appliance that holds one or both sides of the lower jaw forward for some number of months. This can only be successful if the disc can be “recaptured” by the condyle (which can only be seen on MRI but can also be approximated with Joint Vibration Analysis or Doppler).

If the disc cannot be recaptured by the condyle, and the adolescent is still actively growing, surgery is then necessary to reattach the ligaments correctly. If the adolescent is done growing, the opportunity for further growth is limited.
Other Conditions
In addition to “silent” TMJ problems, there are cases of TMJ clicking and popping that need management in the adolescent years. A jaw that gets locked open, or locked closed, is a frightening experience and often points to a disruption of the attachment of the disc to the bones of the TMJ. Failure to manage a jaw joint with a history of being locked will often result in asymmetric function, as the person attempts to simultaneously chew and reduce pain. If this happens during the adolescent growth spurt, growth can be stunted in the body of the mandible.
Though less common in children, pain of the TMJ needs management during the adolescent years. Pain in the jaw is usually muscular rather than bony and can occur for a number of reasons. Asymmetric function, chewing mainly on one side, is a big contributor to pain of the TMJ. People will automatically chew more on the side where the teeth meet better and overuse of one side for chewing will often cause pain in the underused side.
